Article Text

Abstract
Autoantibodies can be an important indicator of paediatric rheumatic disease and useful in establishing a diagnosis. However, autoantibodies may be requested in cases where the patient does not have clinical features strongly suggestive of a rheumatic disease. This can lead to further unnecessary investigations, specialist referral and undue anxiety for the family. The aim of this article is to provide guidance for when it is appropriate to request autoantibodies, which ones to perform and how to interpret the results.
- Paediatrics
- Rheumatology
- Child Health
- Adolescent Health
Statistics from Altmetric.com
Introduction
Careful history and physical examination are of the utmost importance in the evaluation of suspected paediatric rheumatic disease. Once a list of differential diagnoses has been determined, appropriate laboratory tests may be helpful. There are no good screening tests for rheumatic diseases in childhood. However, autoantibodies can provide a powerful guide for diagnosis, and can also provide information on prognosis, disease activity and influence choice of treatment. Autoantibodies should always be requested to support your clinical impression. A positive autoantibody result may be present in other autoimmune diseases, some infections and in healthy individuals.
Improper use of these investigations may result in misdiagnosis, over investigation and wasted healthcare resources.1 For example, antinuclear antibodies (ANAs) are often requested in a child presenting with musculoskeletal complaints without an otherwise strong suspicion for rheumatic disease. An ANA performed in this context may lead to one of two outcomes: the test is negative, and this result does not influence your management, or the test is positive, leading to a more detailed history and examination (which should have been done prior to testing). If the patient is then not diagnosed with a rheumatic disease, this may have caused undue anxiety for the family, preventable investigations and unnecessary specialist referral to a rheumatology clinic.
Physiological background
Autoantibodies are abnormal antibodies produced by pathogenic B cells in response to self-antigens.2 An immune complex is formed from autoantibodies, self-antigens and other immune factors. The immune complex is then deposited in tissues and results in dysfunction or destruction of multiple organs.3 This is demonstrated in figure 1.
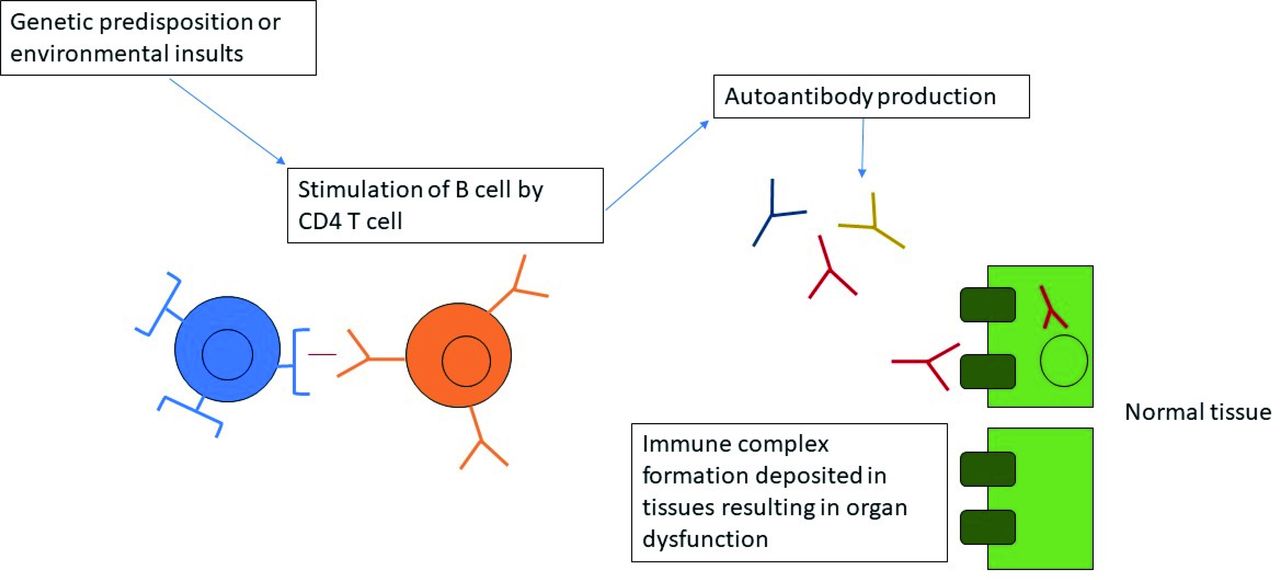
Generation of autoantibodies.
Autoantibodies are often considered an indicator of autoimmune diseases that are characterised by chronic, systemic, excessive immune activation and inflammation, and can affect multiple systems within the body.3 Autoantibodies and their associations in paediatric rheumatic disease are demonstrated in table 1.
Autoantibodies, their associations in paediatric rheumatic disease, cost and turnaround time
Technological background
How are autoantibodies measured?
Antinuclear antibodies
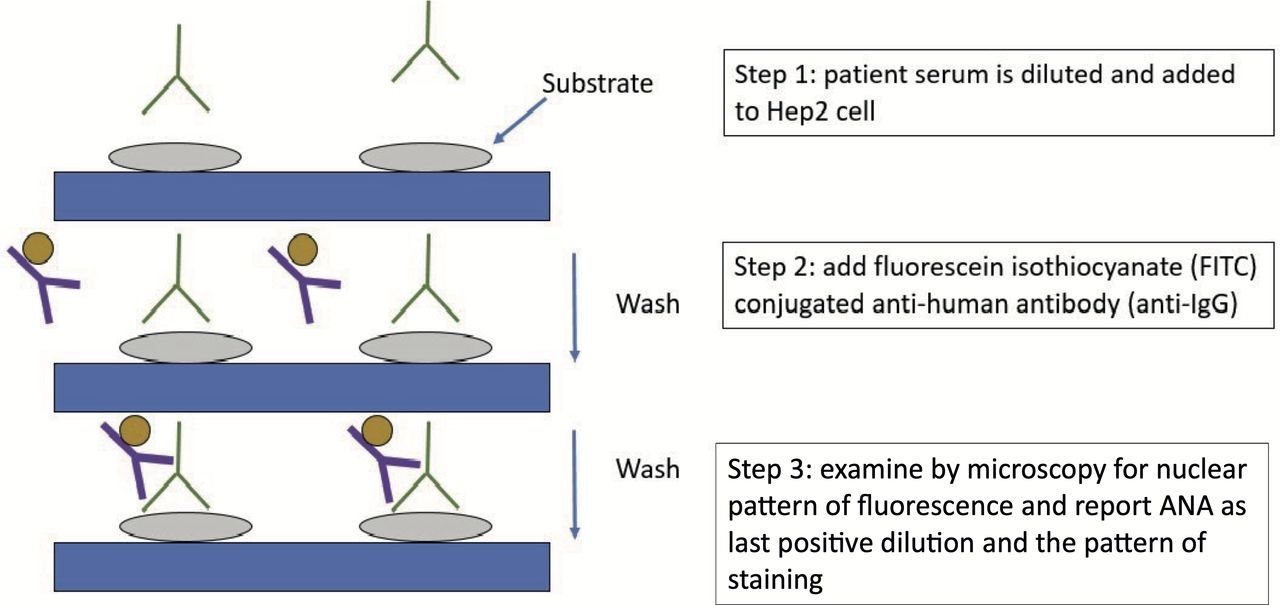
Indirect immunofluorescence (IIF) is a good screening test as it enables the identification of ANA. The gold standard to detect ANA is IIF microscopy on Hep2 cell line, which originates from human tissue.4 This process is demonstrated in figure 2. This requires specialist laboratory expertise to interpret. Alternative methodologies for ANA screening include screening ELISA, fluorescence enzyme immunoassay (FEIA) and multiplex bead-based technology. There are significant differences in the value of each of these methods in terms of cost, turnaround time, expertise required, and sensitivity and specificity.
{kind=link}
{kind=link}
Detection of antinuclear antibodies (ANA) by indirect immunofluorescence.
ANA testing gives two results: the titre and pattern.
ANA titre
In order to reduce the number of false-positive ANA tests, most laboratories report titres. This is the highest dilution of test serum that allows immunofluorescent staining.1 First of all, an ANA screen on Hep2 cells is performed and the patient sample is diluted at 1:80. If the ANA screen is positive, then ANA titration on Hep2 cells is done and the sample is diluted at 1:160, 1:640 and 1:2560.
A positive test result is typically only reported when immunofluorescent staining persists at 1:80 or higher. Many laboratories will then automatically carry out extractable nuclear antigens (ENAs) and double-stranded DNA (dsDNA) autoantibodies in all new positive ANAs with titre of 1:160 or more.5
ANA pattern
The pattern of fluorescence seen in ANA can be associated with particular autoantibodies:
Homogeneous pattern: This can be due to anti-dsDNA or anti-histone autoantibodies, and can be seen in juvenile systemic lupus erythematosus (JSLE) or other connective tissue diseases.
Speckled pattern: This can be due to ENAs, including anti-Ro, anti-La, anti-Smith, RNP and Scl-70. This pattern can be associated with JSLE, mixed connective tissue disease (MCTD), Sjögren’s and systemic sclerosis.
Nucleolar pattern: This can be seen in systemic sclerosis.6
When laboratory staff are analysing these samples, it is essential that as much clinical information as possible is provided. This helps to ensure accurate interpretation of the patient’s sample.
Anti-neutrophil cytoplasm antibodies
Anti-neutrophil cytoplasm antibodies (ANCA) is tested by indirect immunofluorescence on ethanol fixed human neutrophil slides.5 There are two major ANCA patterns: cytoplasmic ANCA (c-ANCA) and perinuclear ANCA (p-ANCA).7
Using ELISA testing, c-ANCA nearly always reacts with proteinase 3 (PR3). Granulomatosis with polyangiitis (GPA, formally known as Wegener’s granulomatosis) is associated with c-ANCA. c-ANCA is very specific for GPA and occurs in more than 80% of cases.6
The major p-ANCA target is myeloperoxidase (MPO). Microscopic polyangiitis (MPA) and eosinophilic granulomatosis with polyangiitis (EGPA, formally known as Churg-Strauss syndrome) are associated with p-ANCA and with MPO on ELISA.
In atypical ANCA, the immunofluorescence test is positive (mostly p-ANCA), but the ELISA for both MPO and PR3 is negative.
MPO and PR3 are tested by FEIA. MPO and PR3 are often tested first by laboratories and ANCA will then be done for confirmatory testing in cases of positive MPO and PR3 antibodies.5
Rheumatoid factor
Rheumatoid factor (RF) refers to a group of antibodies whose antigen binding sites are specific for the fragment crystallisable (FC) portion of IgG molecules. RF is tested by latex-enhanced turbidimetry. The RF reagent is a suspension of polystyrene latex particles of uniform size coated with human immunoglobulin. When a sample containing RF is mixed with the reagent, agglutination occurs, which can be measured by turbidimetry.8
Anti-cyclic citrullinated peptide
Anti-cyclic citrullinated peptide (anti-CCP) is measured by FEIA.
Extractable nuclear antigens
Extractable nuclear antigen (ENA) is measured by FEIA. If the ENA screen is positive, the sample will be tested for each individual ENA identity.
dsDNA antibodies
FEIA is used to screen samples for dsDNA, then Crithidia indirect immunofluorescence is used for confirmation of new positives.5 This uses the haemoflagellate, Crithidia lucilae, as a substrate. This single cell organism possesses a highly condensed mass of circular dsDNA. This acts as a sensitive and specific substrate for detecting autoantibodies to dsDNA.
Indications and limitations
Antinuclear antibodies
ANA is highly sensitive (>95%) and specific (90%) for JSLE,6 and should be requested if the clinician has reasonable suspicion for JSLE based on clinical evaluation.9 However, ANA should not be requested for random screening for JSLE as a positive ANA can occur in a variety of clinical settings, including in healthy individuals. Approximately 20% of healthy people have an ANA of 1:40 or higher, and approximately 5% have an ANA of 1:160 or higher.1 Most children who are ANA positive without signs of rheumatic disease will not go on to develop an autoimmune disease later in life.6
The clinical manifestations of JSLE are diverse and can affect every organ system in varying severities, unique to every individual as shown in table 2.9
Paediatric rheumatic diseases and their typical signs, symptoms, laboratory findings and relevant autoantibodies
A positive ANA is also associated with other autoimmune diseases such as JDM, MCTD, scleroderma, Sjögren’s, autoimmune hepatitis, inflammatory bowel disease, autoimmune thyroiditis and pulmonary fibrosis.9 It can also be present in infections such as tuberculosis, schistosomiasis and parvovirus.
A positive ANA may contribute to a clinical impression of juvenile idiopathic arthritis (JIA), but a diagnosis of JIA should not be based on this alone. A diagnosis of JIA is a diagnosis of exclusion, and a broad differential diagnosis should be considered, including infection, malignancy, other multisystemic rheumatic disease or an autoinflammatory disorder. For example, in the context of a high titre positive ANA in a patient with arthritis, a diagnosis of a connective tissue disease should be considered.
Anti-neutrophil cytoplasmic antibodies
Anti-neutrophil cytoplasmic antibodies (ANCA) is most commonly positive in small vessel vasculitis. ANCA-associated vasculitides (AAV) include GPA, MPA and EGPA.10
The clinical features of AAV are broad, from isolated cutaneous involvement to multisystemic disease. When considering a diagnosis of AAV, it is important to consider other diagnoses such as infection, thrombotic disorders and malignancy. Table 2 includes signs, symptoms and laboratory findings seen in AAV.
It has been well described that there are ANCA negative forms of GPA, MPA, renal-limited vasculitis and EGPA.
It may be appropriate to consider testing patients for ANCA, MPO and PR3 in patients with these features:
Cutaneous vasculitis with systemic features.
Worsening glomerulonephritis.
Pulmonary haemorrhage.
Multiple lung nodules.
Chronic destructive disease of the upper airways.
Long-standing sinusitis or otitis media.
Subglottic tracheal stenosis.
Mononeuritis multiplex or peripheral neuropathy.
Retro-orbital mass—proptosis can be caused by granulomatous malformation within the orbit (pseudotumour).
Scleritis.
It is important to note that ANCA can also be positive in chronic infections and malignancy, such as tuberculosis, HIV and Hodgkin’s lymphoma.2
Rheumatoid factor
RF does not have much diagnostic significance in paediatric rheumatology, apart from aiding in classification of polyarticular JIA (about 5%–10% of polyarticular JIA are positive for RF).6
In children with polyarticular JIA, a positive RF confers a higher risk of aggressive disease. It correlates with longer disease duration, involvement of symmetrical small and large joints and poorer function. RF positive polyarticular JIA is recognised as the paediatric form of adult rheumatoid arthritis (RA). RF positivity aids in therapeutic decisions and use of aggressive immunosuppressant therapy in order to prevent long-term morbidity.2
RF can also be positive in other autoimmune diseases, such as JSLE and Sjögren’s, infections such as tuberculosis and Lyme disease and otherwise well individuals.9
Anti-cyclic citrullinated peptide
Anti-cyclic citrullinated peptide (anti-CCP) is not routinely tested in all children with JIA, but it can be useful in patients with polyarticular disease pattern. As with RF, positive anti-CCP confers a more aggressive disease course in polyarticular JIA and predicts a disease pattern similar to adult RA.
Extractable nuclear antigens
Laboratories will often routinely perform an ENA on any new positive ANA, that is, ≥1:160.5 ENAs performed by laboratories include the following:
Anti-Ro and anti-La: These are associated with JSLE (sensitivity 15%–33%),6 neonatal lupus, Sjögren’s, are involved in the pathogenesis of congenital heart block and may be detectable in ANA negative lupus.
Anti-RNP: This is highly sensitive (>95%) and specific (98%) for MCTD. It can also be present in JSLE and is associated with lupus nephritis.6
Anti-Smith: This is highly specific for JSLE (99%), but is not sensitive (present in only 20% of patients with JSLE).6
Scl-70: This is seen in patients with systemic sclerosis (sensitivity 34% and specificity 99.6%).11
Ribosomal P: This is very specific for JSLE (98%)12 but is only seen in a few patients (sensitivity 23.5%).12 It is associated with lupus with neuropsychiatric features.6
Anti-centromere: This is characteristic of CREST syndrome, a variant of systemic sclerosis (sensitivity 65% and specificity 99.9%).11 There is limited skin involvement but there is association with Calcinosis, Raynaud’s phenomenon, oEsophageal immobility, Sclerodactyly and Telangectasia.
dsDNA antibodies
The presence of dsDNA antibodies strongly indicates JSLE, with a specificity of 84%–95%.6 In most laboratories, all positive ANA results with titres greater than 1:160 will be tested for dsDNA. It is important to consider that the absence of dsDNA does not rule out the possibility of JSLE. dsDNA is used as a marker of disease activity and for monitoring of patients with JSLE, and high titres of dsDNA can be seen in lupus nephritis.
Negative autoantibody tests
Repeating a negative autoantibody test in suspected paediatric rheumatic disease is rarely required, as repeating the test will add little in altering the diagnosis.13 If the clinician has ongoing suspicion regarding a diagnosis where there are evolving signs and symptoms, the test may be repeated after a reasonable time period. In practice, for example, a negative ANA may be repeated after about a year.
Topics for further research
There are no good screening tests available for the diagnosis of paediatric rheumatic diseases, some of which are rare and present with a diverse range of signs and symptoms. A careful history and clinical examination will always be of the utmost importance. With clinical experience comes pattern recognition, and a single biomarker is unlikely to be found to replace this.
Search strategy
A literature search for original articles and abstracts was carried out on the Medline Database via PubMed. An advanced search was carried out using the following search terms: ‘autoantibodies’, ‘paediatric’, ‘childhood’, ‘juvenile’, ‘rheumatology’, ‘rheumatic’, ‘ANA’, ‘ANCA’, ‘rheumatoid factor’, ‘ENA’, ‘anti-RNP’, ‘anti-Smith’, ‘anti-Ro’, ‘anti-La’, systemic lupus erythematosus’, ‘mixed connective tissue disease’, ‘dermatomyositis’, ‘juvenile idiopathic arthritis’, ‘scleroderma’, ‘systemic sclerosis’.
Clinical bottom line
Autoantibody testing should be requested judiciously and only when there is a strong clinical suspicion for a rheumatic condition.
Autoantibody results should always be interpreted within the clinical context and should be used to support your clinical impression.
Test your knowledge
An 8-year-old girl is referred to your clinic with pain in her knees and ankles. Her GP has done some baseline bloods and she has a positive ANA of 1:80. She is a keen gymnast and her pain is worse on exertion. She is otherwise well. On examination, she is hypermobile and has a Beighton score of 8/9. The rest of her examination is normal. What do you do next?
Send blood for FBC, ESR and CRP.
Check other autoantibodies including RF, ENA and dsDNA.
Refer to rheumatology clinic.
Reassure and refer to physiotherapy.
You see an 11-year-old girl in clinic who has been complaining of pain in her knees and backs of her legs for 6 months. She has been increasingly tired and is struggling to concentrate at school. On examination, she has warm effusions over both knees. You notice she has a malar rash across her cheeks and has some oral ulcers. What do you do next?
Check autoantibodies including ANA, ENA, dsDNA, anticardiolipin antibody and lupus anticoagulant.
Check urinalysis and send for urine protein:creatinine ratio.
Check bloods for FBC, film, ESR, U+E, LFT, CRP, bone profile, complement, ferritin, iron studies, immunoglobulins and TFTs.
Check her BP.
All of the above.
What is the gold standard test for detecting ANA?
Indirect immunofluorescence (IIF) on Hep2 cell line
Fluorescence enzyme immunoassay (FEIA)
ELISA
Indirect immunofluorescence (IIF) on ethanol fixed human neutrophil slides
Which of the following conditions are associated with c-ANCA and PR3?
Microscopic polyangiitis (MPA)
Granulomatosis with polyangiitis (GPA)
Juvenile dermatomyositis (JDM)
Eosinophilic granulomatosis with polyangiitis (EGPA)
What condition is anti-RNP specific for?
JSLE
JDM
MCTD
Systemic sclerosis
Localised scleroderma
Answers to the quiz are at the end of the references.
Answers to the multiple choice questions
D
E
A
B
C
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
With thanks to the immunology laboratory staff at the Queen Elizabeth University Hospital, Glasgow. In particular, thank you to Dr Lauren Hennessy and Dr Moira Thomas.
Footnotes
Contributors JK was the main author of this paper. RMB and JW contributed to the planning of this paper and revised the paper critically.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.